*Updated 3.20.13 (Ellie is 3.5 years old)*
So What Exactly Is SPD?
If you happen to be like me, Sensory Processing Disorder [SPD] is a new experience and a bit confusing. Okay, it is really confusing. As you start to read all of the checklists and behaviors that might be associated with said disorder, you start to think “hey, I have that.” or “OMG, my child has that for sure!”. The fact of the matter is that everyone has some of the behaviors on the checklists and that is absolutely typical. It is true. What makes it a disorder is that it affects one’s ability to complete tasks, learn, and / or communicate. The sensory issues are so severe that they impact daily activities of living [ADL].
History:
While SPD may seem like a relatively new phenomenon, it was studied by Dr. Anna Jean Ayred, PhD, OTR since the 1960s where she coined the term “sensory integration dysfunction”.
Ever hear of the book “The Out-Of-Sync Child” by Carol Stock Kranowitz from 1995? This author touches on SPD and that was in the mid-1990’s.
Since then, starting around 2007, Sensory Processing Disorder and Sensory Integration Disorder have become more widely studied. HOWEVER, there is no actual ICD-9 medical code for SPD. . . YET. An ICD-9 is a diagnostic code used by medical providers, OTs, etc. For example, Down Syndrome has a ICD-9 code of 758.0 Without an ICD-9 code, billing to insurance and obtaining therapies is rather difficult.
How is it that a disorder that has been around for over 50 years does not even have its own diagnostic code? How is it that there is no definitive diagnostic tool for SPD?
The Senses and the Process:
Many of us know the most common senses of taste, smell, touch, auditory (hearing), and visual, but there are also other senses such as body position in space, movement/vestibular. These senses are all translated by receptors in the body (ie skin, muscles, tongue, tendons,) that send signals to the brain. Yep, the nervous system. The thing with SPD, is that these sensory pathways are not functioning properly. The sensory impulses are not relayed to the brain as they should be.
Hypo Vs. Hyper Sensitivity:
Now, not all of the senses are affected. For some people, tactile is the main sense affected for others it is visual and auditory. Some people are hypo-sensitive (ie indifferent to pain, temperature, touch, sounds) and some may be hyper-sensitive (pulling back from touch or covering ears due to loud noises or covering the eyes from bright lights). In fact, those with SPD can have BOTH hypo- and hyper-sensitivity.
For instance, Ellie is hyper-sensitive with her face and head. She throws a huge conniption fit if her face is being washed or if her head gets wet. Bath-time was hell on Earth. We probably had the filthiest baby ever because bath time = Bear Torture Time.
The rest of her body and her mouth are predominantly hypo-sensitive as in she is always insensory craving state with her mouth. Something such as a toy, clothing, lovie, teether, paper, toothbrush, you-name-it is always in her mouth. She eats chalk, crayons, pencils, and even board books.
She also craves motion--the rocking, the swinging, the bouncing as well as the movement of HEAVY objects. That all involves the touch / tactile sense. She also has some vestibularissues--she is clumsy. She falls a lot and at times, it looks as though she is trying to walk straight, but ends up going to the left (or right). Her muscles, joints, tendons, and ligaments are not working in sink with her brain.
Typical Questions:
So how is it a disorder?
Some of these things every kid does so how is Ellie different?
She is developmentally delayed so doesn’t some of this make sense?
Don’t most toddlers have bouts of clumsiness and falling?
Don’t many kids like to mouth things?
What child does not love to swing or be bounced?
I know. I know. This is why I was so shocked and why I sought 2nd and 3rd opinions. Come on! Most of this sounds typical to me. Well, not the crazy bath stuff (it was getting dangerous with her trying to escape. Oh and the screaming!). Not to mention her oral fixation. Still, much of this seems typical to me.
Sensory Issues vs. Sensory Processing Disorder:
The fact of the matter is this: it IS typical UNLESS it impairs social interaction, learning, communication, and/or play (work).
For my daughter, it IS affecting her learning, communication, and socializing.
 |
| Chewelry |
Our Current Therapy for Oral Sensory Seeking:
Mouthing Objects: Think Outside the Box for Oral Sensory Seeking
Chewy Tubes for Oral Stimulation, Oral Aversion, Speech, and Eating
(This is a comprehensive review of the various chewy tubes that we have used with Ellie.)
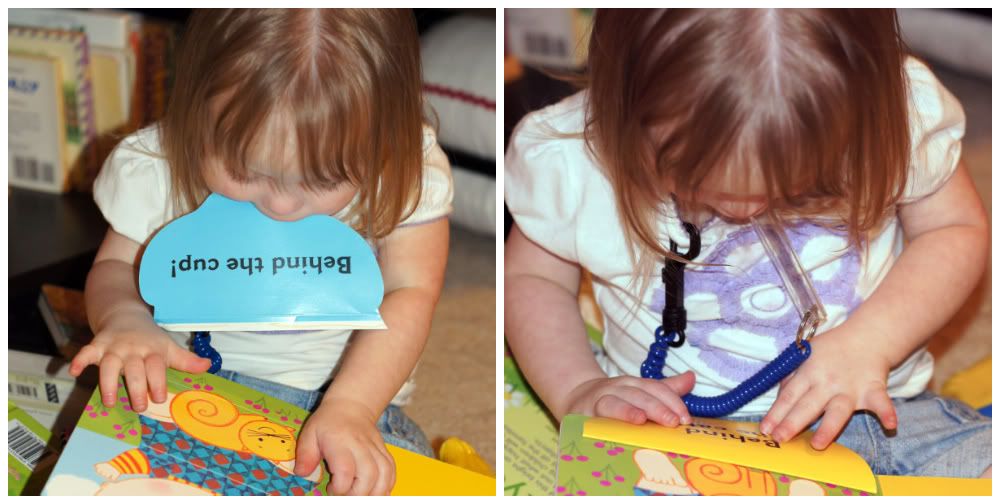 |
| Left: Sensory seeking and destroying the book. Right: Substituted Chewlery to relieve oral sensory craving |
Food with High Sensory Input:
Sensory foods are foods that are going to give intense oral input, i.e. sour, spicy, cold etc:
Lemons
Limes
Sour fruit sticks--Target has these cherry lime ones
Dried fruit
Peppered Beef Jerky
Lemons
Limes
Sour fruit sticks--Target has these cherry lime ones
Dried fruit
Peppered Beef Jerky
COLD foods--try refrigerating fruit snacks or the fruit twists
Frozen peas
 |
| Just some suggestions that are Ellie-specific recommended by her therapist |
 |
| Ellie is eating peppered beef jerky. Notice that her Chewelry is attached to her shirt and she is holding her lovie in her other hand. This girl has a whole arsenal of chews for sensory oral stimulation! |
Heavy Work for Sensory Integration
Heavy Work Backpack Tutorial


 |
| You can even use the weighted backpack and the weighted sock-snake to create a "heavy work" cart/stroller. |
Coming Soon. . . Typical Treatments and Resources
